Eighty Hours in Trauma Surgery
I'm writing this from my car.
It's half past six on a Wednesday evening, and I'm sitting in the hospital car park finally eating the sandwiches I made for lunch this morning: sourdough bread with butter, marmite, and brie, and another with strawberry jam instead of the marmite. The bread has cranberries and hazelnuts baked into it. I made these sandwiches at six a.m. this morning. It is now a quarter past six in the evening.
How We Got Here
I'm in my second week of my surgical rotation but last week barely counts; I only had two days of surgery. I was on call for Obstetrics and Gynaecology on Good Friday and Easter Monday, and thus missed the surgical orientation on Tuesday morning while finishing up a Caesarean section and doing a ward round in the post-natal ward at Edendale Hospital.
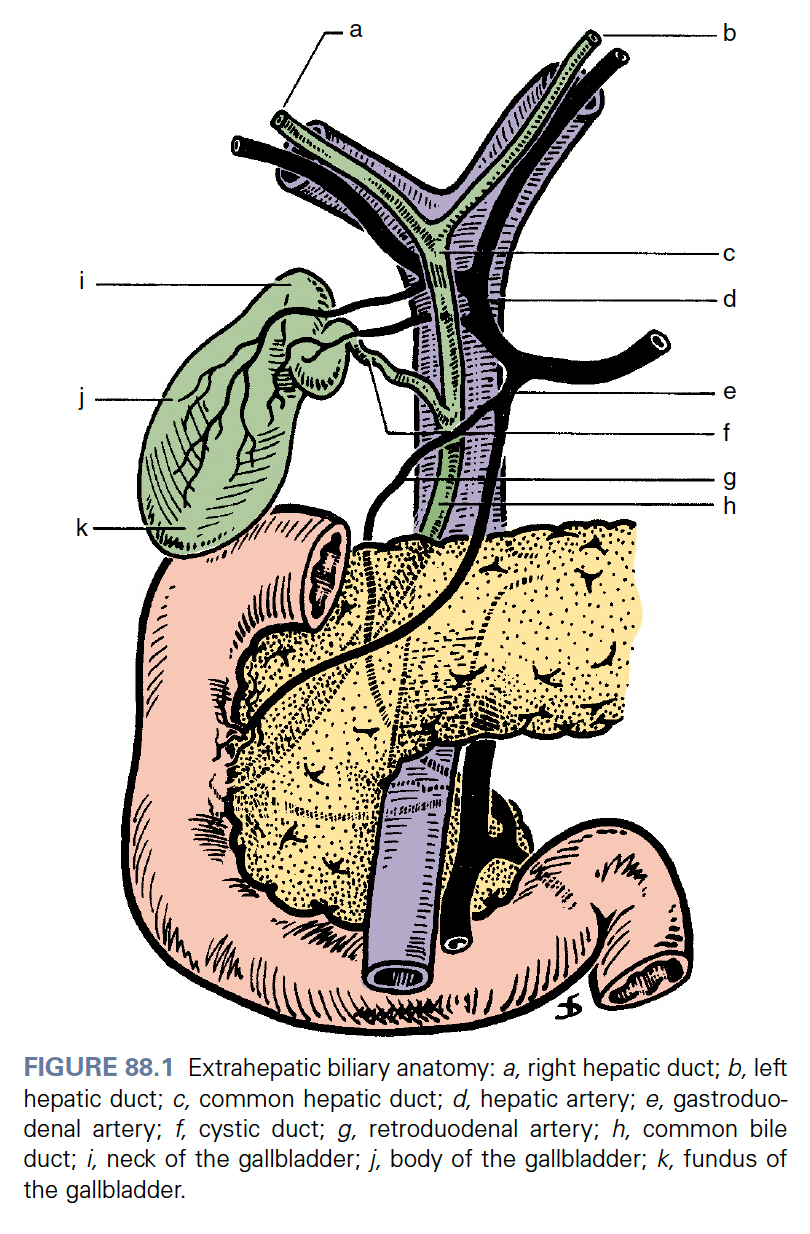
I then spent Wednesday and Thursday in the surgical outpatient department. Wednesday was the breast, endocrine and soft tissue clinic and I mainly saw patients who had had previous total thyroidectomies or lobectomies. And Thursday was the hepatobiliary clinic which mainly involved seeing patients who were to be admitted to undergo endoscopic retrograde cholangiopancreatography: this procedure is very descriptively named and involves the passage of a camera tipped tube, an endoscope with a side port, down the oesophagus, through the stomach and into the second part of the duodenum where the ampulla of Vater, the common conduit at the terminal ends of the main pancreatic duct and the common bile duct opens into the intestine. The ampulla is then intubated and a contrast medium is injected into the biliary tree and fluoroscopic imaging is used to delineate the biliary anatomy and look for pathology.
Anyway I am getting side-tracked. After admitting the first couple of patients for this procedure we received word that we would have to cancel all those procedures scheduled for the next day due to a lack of equipment. I tried my best not to think about the effort and the distance travelled and the expense incurred by our indigent patients only to hear that they couldn't be helped.
After 16h00 on Thursday I went to casualty for my first surgical call at Greys. It was a bit of a blur but I had very competent and friendly seniors. Admitting patients on the surgical patient electronic database does become rather tedious at 3 a.m. in the morning, but at least I started to get the hang of it. The knowledge that I was going to the Western Cape for the weekend for Renier and Zelmi's wedding the next day was good motivation to push through.
I was fortunate that my dad could give me a lift for the ninety minute drive to the airport where I was able to check in my luggage with about 60 seconds to spare before bag drop closed. I got just enough sleep in the car ride to the airport and on the plane to ready me for the two-and-a-half hour drive to the wedding venue that evening. I arrived pretty exhausted, but it was wonderful to see so many close friends for the first time in several months and exchange stories of our new lives around the bonfire while getting ready for the big day.

This week, I'm on trauma surgery. After an exciting and not very restful weekend, having to cover a call on Monday for one of my colleagues who had fallen ill with pneumonia was not ideal. After the handover meeting I was given a list of 6 wards to systematically go through to find and see all the trauma patients. After the consultant ward round at about midday, it was my duty to carry out all the plans. By 16h00, I wasn't close to done so perhaps it was fortunate that I was on call, so I could just carry on working. There was a steady flow of tasks to complete and it seemed as though as soon as I was getting close to having done everything, I would get a phone call from another ward asking to resite two more IV lines or to come and review a patient who was projectile vomiting. It took me a long time and a lot of physical effort to hold down and cannulate a 3 year old boy admitted for a cytotoxic snakebite. In the end, I went for the external jugular vein; something I've seen several times on paediatric rotations, but never actually done before. You have to learn quickly when it's your job.
Around midnight, I found some time to tuck into a venison pie from Peregrine Farm Stall. After travelling a thousand kilometres and being in a cooler box in my car all day, it was still far superior to all the garage pies I have had on call this year.
CRUSH Syndrome
The most common condition of trauma patients admitted this week is Crush syndrome.
The classical description involves someone trapped under rubble after an earthquake: the muscles are compressed for a prolonged period, the cells are damaged, and when the pressure is finally released, myoglobin and other intracellular contents like potassium and creatine kinase floods into the bloodstream. Myoglobin is a large molecule that the kidneys struggle to filter. It precipitates in the renal tubules and causes acute kidney injury. In South Africa the inciting trauma is almost invariably community assault, often with a sjambok, rather than an earthquake.
Treatment is aggressive IV fluid resuscitation; litres and litres to flush the myoglobin through the tubules before they obstruct. Urine output is monitored obsessively. In severe cases, urinary alkalinisation and dialysis may be needed especially if pulmonary oedema develops which is not unlikely when you give these volumes of fluid. So crush syndrome is really a condition that bridges trauma, nephrology, and social medicine all at once.
The Call That Ended the Week
Friday night was busy. I was on call in casualty. We admitted seven patients: two traumatic brain injuries, a perforated abdominal viscus with the classic free air under the diaphragm on chest X-ray, and two cases of what appeared to be appendicitis, and two paediatric surgical patients. One of the appendicitis cases turned out, on laparotomy, to be severe pelvic inflammatory disease, which required urgent consultation with obstetrics and gynaecology in theatre.
At about 03h00, after I had admitted all these patients and the duties in casualty were done for the time being, I joined the intern on call in the wards to help seeing all the surgical patients in the hospital as has to be done over the weekend. While I was drawing some blood from a patient with Crush syndrome, the hospital intercom crackled on: "Can all doctors in the vicinity of [Ward X] please come immediately for a resuscitation."
With the needle I was using safely disposed in the sharps container. I briskly made way to the ward in question expecting there to already be several doctors at the scene.
It was just myself and one other intern at the scene. I hurriedly pulled on some gloves while being shown to the patient. He was an middle aged man, in his fifties perhaps. A urology patient according to label above his bed. He was catheterised, on bladder irrigation with notable macroscopic haematuria. More importantly he looked very dead. The sisters said he was just found unresponsive.
I call out to him while feeling for the carotid pulse. There is no pulse and he is very cold. I start doing chest compressions thinking it is a bit of a futile endeavour. I get the nurses to take the patient's temperature: 33.8 degrees Celsius. Clearly this man has been dead for a while. His pupils are fixed and mid-dilated. The rhythm check when it eventually happens shows asystole as expected. There is no intravenous access. Another intern arrives, I don't know her but I ask her to do a blood gas. By this time, I don't think it's worth trying to establish intravenous access. She struggles, so I get one of the sisters to take over chest compressions and attempt the blood gas myself. I draw the blood from the femoral artery, and it confirms what I had suspected. This patient has been dead for at least an hour or two. Hypostasis or livor mortis, the gravity dependent pooling of blood, has set in. The haematocrit of the blood I have taken is visually very low; clearly the cellular component of the blood has redistributed to more dependent areas. At this point I call the time of death, noticing that some of the facial muscles are already stiff - the start of rigor mortis.
I wash my hands rueing the messy and unnecessary waste of time. At least another doctor is coming to certify the death. There are still so many patients to see before the morning ward round.
I Open at the Close
A few bays later, near the back of one of the wards, I came to a young man. He was 23 or 24, my age. He had Crohn's disease complicated by a large enterocutaneous fistula. The surgeons had attempted to repair it and had been unable to complete the procedure. He was now being managed palliatively.
He was a skeleton. Sitting up in bed, struggling to breathe, trying to sip some water. There was a large dressing on his abdomen, but it doesn't completely cover the fistula. I can see directly into his abdomen; a reddish mess of adhesions enveloping loops of bowel and a steady stream of enteral contents flowing into a bucket. He was dying, and I think he knew it, though I wasn't sure how explicitly anyone had told him.
I sat with him for about half an hour. I told him honestly what I understood about his condition. He thanked me and asked me to help him die.
Holding back unexpected wave of tears, I gently told him that assisted dying is illegal in South Africa. I adjusted some of his medications to try to ensure he wasn't in any pain. I cancelled the blood transfusion that had been scheduled for him; he didn't want any more intervention. I stayed with him a while longer because I couldn't bring myself to leave.
He died that night, or early the next morning. They mentioned it briefly in the Monday handover.
The Tally
That call concluded an eighty-hour week in trauma surgery. Seven admissions in casualty. A futile cardiopulmonary resuscitation. An end-of-life conversation. Thirty-odd patients in the wards seen including all the trauma ward patients: several crush syndrome, multiple traumatic brain injuries, polytrauma from motor vehicle accidents and community assaults, two snakebite patients and some general surgery patients with severe medical problems like diabetic ketoacidosis, and cholangitis.
I got to CrossFit once, came second at a pub quiz, and managed to stay upright throughout. I have a cycling race on Sunday. I haven't raced since April last year so that should be interesting. But after a week like this, sitting on a bike in the sunshine and going nowhere in particular sounds lush.
It's quite interesting work. But it's a pretty tough ask for ~R170 or £7.50 an hour.